

")
")


Medicare
DARZALEX FASPRO® (daratumumab and hyaluronidase-fihj)
Main Menu
Downloadable Forms

- Benefits Investigation FormA way to find out if DARZALEX FASPRO® is covered by the patient's insurance plan, including requirements for coverage or prior authorization, any out-of-pocket costs, and approved pharmacies.
- Bulk Benefits Investigation Guide
 Learn how to submit requests for multiple patients at once in the Provider Portal.
Learn how to submit requests for multiple patients at once in the Provider Portal. - Business Associate Agreement
 Complete a Business Associate Agreement for your practice only once. No individual patient authorizations are required.
Complete a Business Associate Agreement for your practice only once. No individual patient authorizations are required. - Coding & Billing in Hospital Outpatient Departments GuideCoding information to support access & reimbursement for DARZALEX FASPRO®.
- Coding & Billing in Physician Office GuideCoding information to support access & reimbursement for DARZALEX FASPRO®.
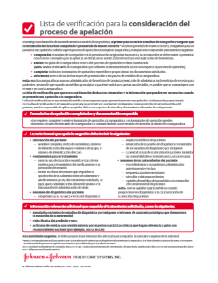
- Exception Considerations Checklist
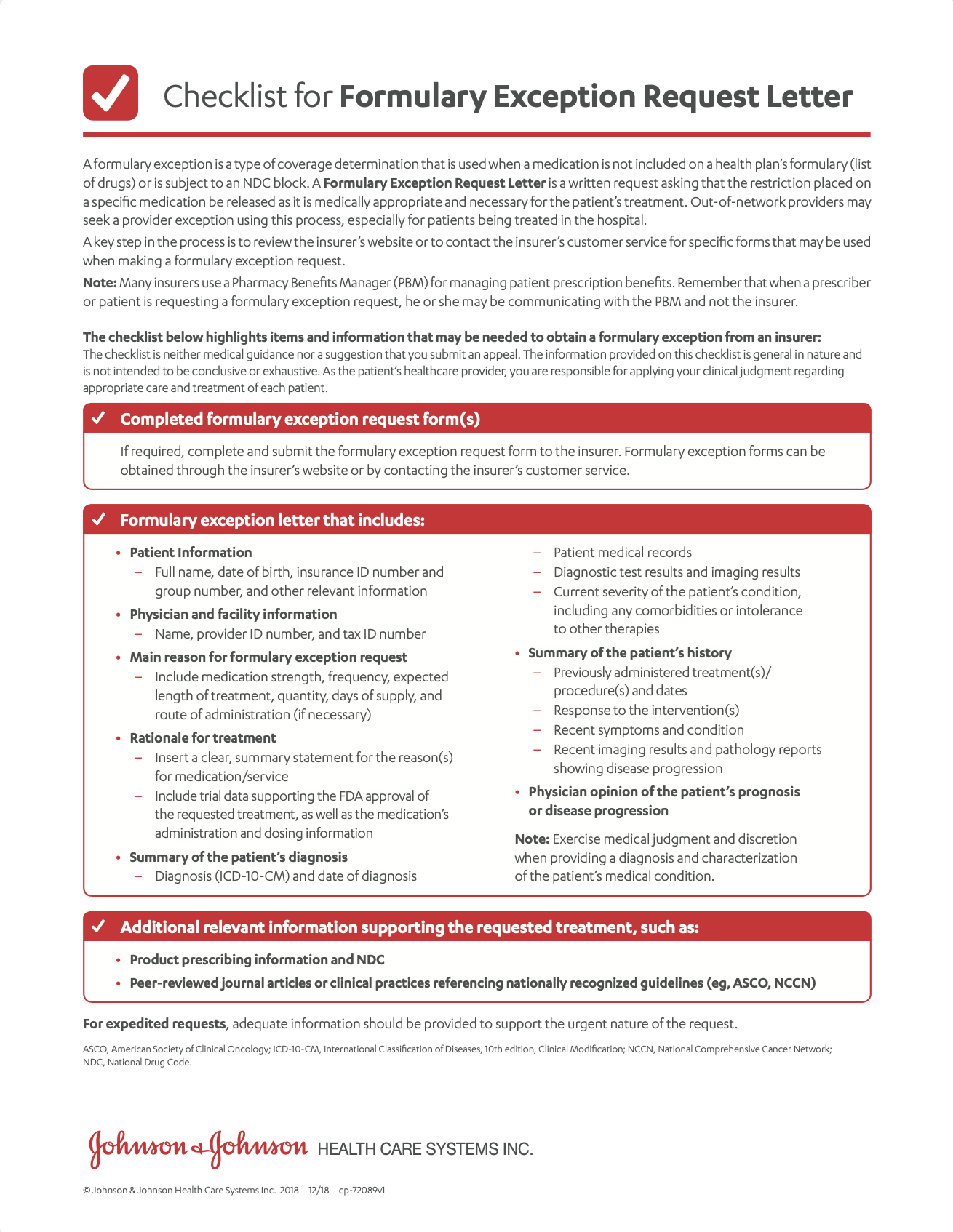 A guide to submitting a formulary exception request.
A guide to submitting a formulary exception request.
Exception Considerations Checklist (en español) - Janssen CarePath Resource GuideA comprehensive summary of support tools for your office to help patients start and stay on treatment.
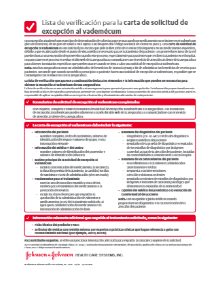
- Letter of Exception
 A template that you can fill out and submit to a patient’s health insurance provider asking them to cover a medication that is not on formulary.
A template that you can fill out and submit to a patient’s health insurance provider asking them to cover a medication that is not on formulary. - Letter of Medical Necessity
 A template that you can fill out and submit to a patient’s health insurance provider. You may use it to explain why DARZALEX FASPRO® is medically necessary for your patient.
A template that you can fill out and submit to a patient’s health insurance provider. You may use it to explain why DARZALEX FASPRO® is medically necessary for your patient. - Patient Account Overview
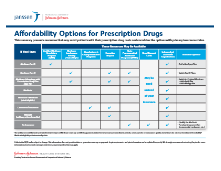
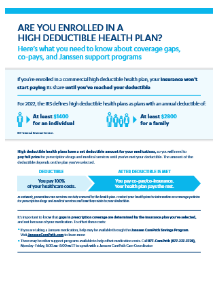
- Patient Affordability OptionsDiscover options that can make DARZALEX FASPRO® more affordable for your patients.
- Patient Authorization FormIndividual patient form for offices without a Business Associate Agreement.
Patient Authorization Form (en español) - Patient Authorization Form (en español)Individual patient form for offices without a Business Associate Agreement.
- Prior Authorization Considerations Checklist
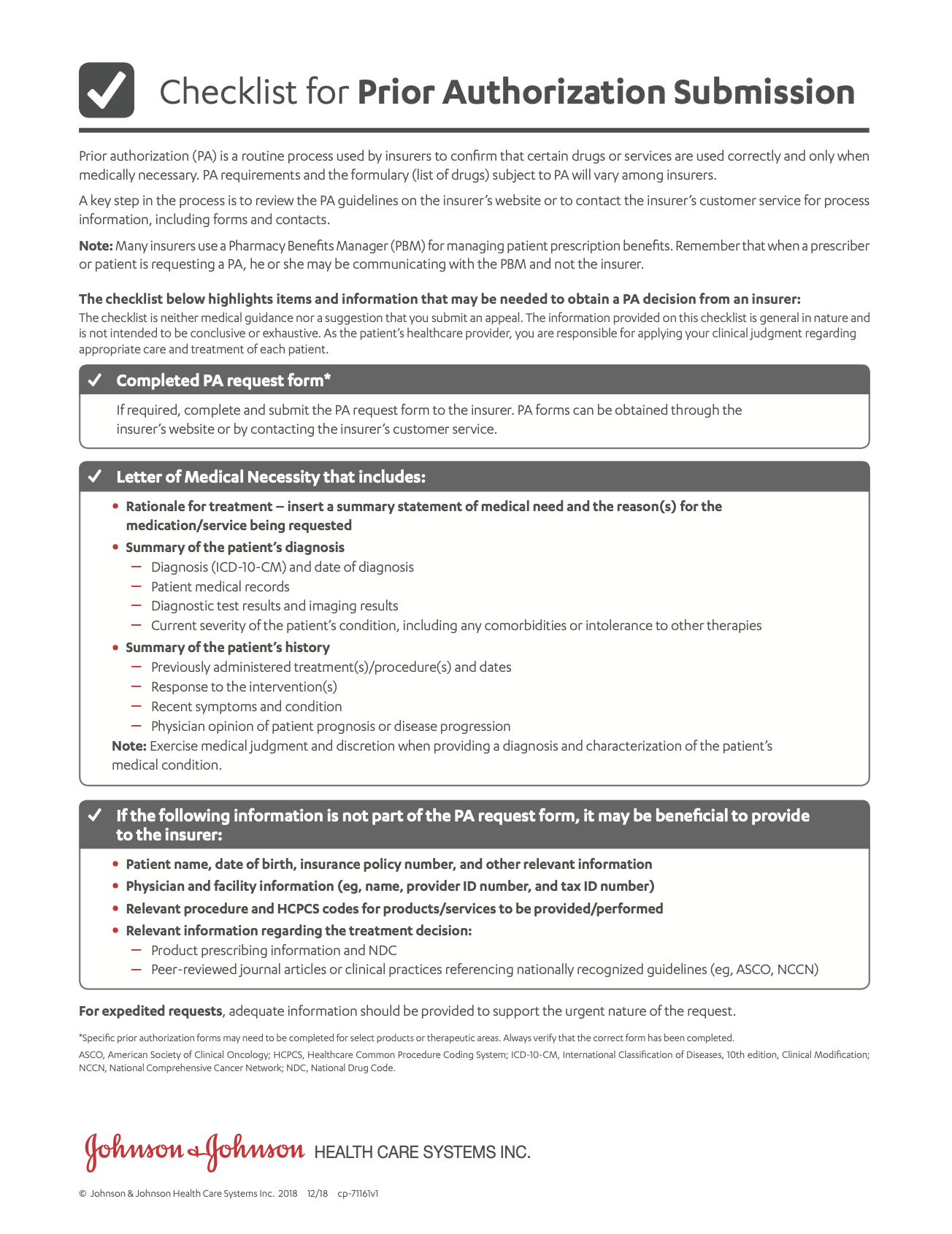 A checklist to guide you through the prior authorization process.
A checklist to guide you through the prior authorization process.
Prior Authorization Considerations Checklist (en español) - Reimbursement & Access Guide
 A comprehensive summary of important medication information including uses, Important Safety Information, access, and reimbursement.
A comprehensive summary of important medication information including uses, Important Safety Information, access, and reimbursement. - Savings Program (Overview)Eligible patients using commercial or private insurance can save on out-of-pocket costs for DARZALEX FASPRO®.
- Savings Program Assignment of Benefits Form
 A form the patient can submit that allows Janssen CarePath Savings Program to reimburse the provider directly.
A form the patient can submit that allows Janssen CarePath Savings Program to reimburse the provider directly. - Savings Program Rebate Form
 A form the patient can submit if the pharmacy is not able to process the Janssen CarePath Savings Program card.
A form the patient can submit if the pharmacy is not able to process the Janssen CarePath Savings Program card. - Savings Program – Submitting Medical ClaimsA guide on submitting medical benefit rebate claims for DARZALEX FASPRO®.
- Verification of Benefits Guide (Medical)
 A guide to understanding the Verification of Benefits for your patient’s medical benefits.
A guide to understanding the Verification of Benefits for your patient’s medical benefits. - Verification of Benefits Guide (Pharmacy)
 A guide to understanding the Verification of Benefits for your patient’s pharmacy benefits.
A guide to understanding the Verification of Benefits for your patient’s pharmacy benefits.
X
Hover on a document on the left for a quick document preview
Medicare
Medicare is a government-funded program that provides healthcare coverage for:
- People over age 65 with a work history
- People with certain disabilities who have been disabled for 2 years or more
- People who have end-stage renal disease (ESRD) or ALS (also called Lou Gehrig's disease)
Medicare is divided into 4 parts: A, B, C, and D.
Part A
Inpatient care in hospitals and skilled nursing facilities; hospice care
Part B
Doctor visits and other outpatient services; medications given by a healthcare provider
Part C
Medicare Advantage Part A and Part B offered by private health plans; most plans include prescription drug coverage
Part D
Prescription drug coverage
While Medicare covers many healthcare needs, it may not cover all the healthcare costs for each patient. The patient may have to pay a monthly premium for Medicare and a co-pay, co-insurance, or deductible.
Janssen CarePath can help Medicare patients with Benefits Investigations, Prior Authorization support, and information on cost support programs.
Learn about the different parts of Medicare. Also see what it may cover, including medications.
Medicare Resource Guide (en español)
Medicare Resource Guide (en español)